Fatty Liver Disease: What Your Diagnosis Actually Means
Written by Tim Dailey Former fine-dining chef · Michelin-starred kitchens · Stage 3 NASH, clinically verified recovery · not a doctor
12 min read
Tim's results (ALT: 127→43, Liver Fat: 65%→<5%, Fibrosis F2→F0) are his own clinically verified outcomes. Individual results vary.
Clinical Quick Answers
What is fatty liver disease?
Fatty liver disease occurs when fat accumulates in more than 5% of liver cells. The non-alcoholic form develops through metabolic dysfunction — primarily insulin resistance — rather than alcohol consumption. It exists on a spectrum from simple fat accumulation (NAFLD) to an inflammatory form with cell damage (NASH). Most people have no symptoms until the condition has progressed significantly.
What causes fatty liver disease in people who don't drink alcohol?
In non-drinkers, fatty liver develops when the liver becomes resistant to insulin and begins converting excess carbohydrates — particularly fructose — into fat through a process called de novo lipogenesis. The liver produces and retains fat it cannot efficiently export. This is why the condition develops in people with no significant alcohol history, and even in people who are not overweight.
What is the difference between NAFLD and NASH?
NAFLD (non-alcoholic fatty liver disease) refers to fat accumulation in the liver without significant inflammation. NASH (non-alcoholic steatohepatitis) is the same fat accumulation combined with liver cell inflammation and damage — a more serious stage that carries higher risk of progression to fibrosis and cirrhosis. Standard blood tests cannot reliably distinguish between them; fibroscan or biopsy is required for accurate staging.
Can fatty liver disease be improved without medication?
Research consistently shows that hepatic steatosis responds to specific nutritional and lifestyle changes. The liver has significant regenerative capacity — studies have documented measurable reductions in liver fat through targeted dietary intervention. The degree and timeline of improvement vary significantly between individuals. No currently approved medication specifically targets fatty liver disease as a first-line treatment.
These answers reflect current research and Tim's documented experience. Individual results vary. This is not medical advice.
The number came back. Nobody explained what drives it.
The appointment lasted twelve minutes. The doctor said the words — fatty liver, elevated enzymes, NAFLD — and then said to lose some weight and come back in six months. The door closed. You are left with a condition name you are about to Google in a car park, a number you do not have a framework for, and a growing suspicion that what you were just told is not the whole picture.
It isn't.
Fatty liver disease is one of the most common chronic liver conditions in the world, affecting an estimated one in four adults globally. Fat accumulated in your liver before there was a single symptom to warn you. Most people find out incidentally — through routine blood work, through a scan ordered for something else, through an elevated result a GP flagged without fully explaining. What they are rarely given, in the time available, is the mechanism. Why this happened. What is actually driving it. And what understanding that mechanism means for everything that comes next.
This article is that explanation.
One specific biological process drives the fat accumulation in non-alcoholic fatty liver disease — and it is not the one most people assume when they first hear the diagnosis. Understanding it changes how you read the condition, what you do about it, and what "monitor and wait" actually means as an instruction.
You may see this condition referred to as MASLD — metabolic dysfunction-associated steatotic liver disease — following a 2023 rename by major international hepatology societies. The underlying biology is the same. This article uses NAFLD and NASH as its primary terms because those are the words most people hear in appointments and search for afterward.
How Fat Accumulates in the Liver — The Mechanism Behind the Diagnosis
The standard explanation for fatty liver disease goes like this: too much dietary fat, too much alcohol, too little movement. The liver becomes overwhelmed. Fat builds up. Change your habits.
That explanation is incomplete. For a significant proportion of people who receive this diagnosis — including people who do not drink, people who are not overweight, and people who have been eating carefully for years — it is actively misleading. It explains the condition by describing its most familiar-looking risk factors. It does not explain the mechanism.
The liver manages fat through four pathways simultaneously: dietary fat arriving from food, fat released from adipose tissue into the bloodstream, fat manufactured by the liver itself, and fat packaged for export out of the liver. In a healthy metabolic state, these pathways stay in dynamic balance. Fat arrives, is processed, is burned for energy or exported, and the liver stays clear. Research published in Cell and Molecular Life Sciences found that hepatic steatosis develops when this balance breaks down — when fat production and uptake exceed the liver's capacity to export and oxidise it, a process driven by metabolic dysfunction rather than by dietary fat intake alone.
The disruption that breaks this balance, in the majority of NAFLD cases, is insulin resistance. Under normal conditions, insulin signals the liver to stop producing glucose and to manage incoming carbohydrates efficiently. When cells throughout the body become resistant to those signals, the liver compensates — and compensates badly. It upregulates a pathway called de novo lipogenesis: the manufacture of fat from carbohydrates, specifically from fructose, rather than from dietary fat. The liver is not storing the fat you eat. It is producing fat from carbohydrate inputs it can no longer process and clear, and it is storing that fat in hepatocytes — liver cells — rather than packaging and exporting it. Research examining the molecular mechanisms of hepatic fat accumulation in NAFLD identifies upregulated de novo lipogenesis and reduced fatty acid oxidation as the two primary drivers of fat retention in affected livers.
This is why elevated liver enzymes — particularly ALT — are often the earliest detectable signal the process is underway, sometimes years before imaging shows visible fat deposits. Understanding [what an elevated ALT result actually indicates] in this context puts the number in a different frame than the one most twelve-minute appointments provide.
It is also why the condition develops silently. De novo lipogenesis runs on metabolic signals, not on symptoms. Fat accumulates in hepatocytes over months and years without any physical indicator — which is [why most people have no symptoms until the condition progresses] to a point where the liver is under significant metabolic stress. By the time a blood test flags something, the process has often been running for a considerable time.
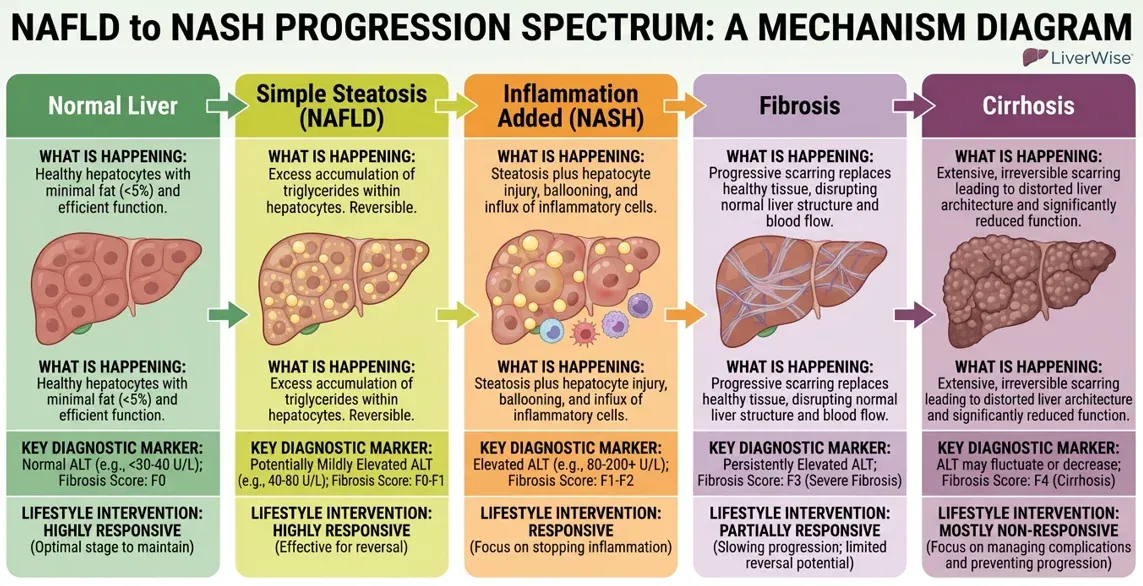
The spectrum from simple fat accumulation to serious liver disease runs in a specific progression. At one end: normal liver tissue. Then simple steatosis — fat in the liver, no significant inflammation. Then NASH: the same fat accumulation, with the immune system engaged, causing active inflammation and cell damage. Then fibrosis — scarring of liver tissue as the immune response becomes chronic. Then, at the furthest progression, cirrhosis. Research on the pathophysiology of this condition is consistent on one central point: the distinction between simple steatosis and NASH is an inflammatory one.
Fat in the liver becomes a different clinical problem when the immune system engages — and that engagement changes the risk trajectory significantly. [The difference between NAFLD and NASH, and why staging matters] is covered in full elsewhere in this site. What matters here is that the diagnosis you received is a point on a spectrum, not a verdict, and that understanding which point determines what the next move is.
The First Step
The mechanism your doctor didn't have time to explain is in the article. The first thing to do about it is in this.
The 72-Hour Emergency Protocol. Enter your email and I'll send it now. Free.
What I Found When the Labs Came Back Six Years After I Stopped Drinking
I was diagnosed with Stage 3 NASH after six years of sobriety.
I want to stay with that sentence for a moment, because it contains the most important thing I can tell anyone who has just received this diagnosis and is trying to understand how they got here.
Six years. No alcohol. I had rebuilt my diet — as a former professional chef who had worked in Michelin-starred kitchens and spent twenty years thinking seriously about food, I was not careless about what I ate. I moved. The standard list of risk factors, as I understood them, did not describe my life. And the labs came back showing significant liver disease anyway.
I sat in the car park after that appointment with a number I did not know how to hold. It was not, in that moment, a statistic. It was the sound of the door closing on a version of what I thought my life looked like.
What I came to understand — after eight months working through the peer-reviewed hepatology literature, looking for the mechanism nobody had explained — was that the condition had been running on metabolic rails that had nothing to do with alcohol. De novo lipogenesis does not require alcohol to activate. It requires insulin resistance, excess carbohydrate inputs the liver cannot process efficiently, and time. I had been supplying all three without knowing it. The six years of sobriety was not irrelevant to my health in other ways. It was entirely irrelevant to the specific mechanism that had been accumulating fat in my hepatocytes for years before the lab flagged it.
This is not an unusual story. It is, in fact, the story of many people who receive this diagnosis. The alcohol assumption — the persistent idea that fatty liver disease is something that happens to heavy drinkers — is the most common and most damaging misconception in public understanding of this condition. It causes shame that has no clinical basis. It causes confusion in people who have done everything they were told was the right thing and still received this diagnosis. And it misdirects attention away from the mechanism that is actually driving the fat accumulation.
The full documented account of what happened after that car park — the specific interventions, the clinical findings, the twelve-month timeline — is in [Tim's documented experience with Stage 3 NASH]. What matters for this article is simpler: the condition is metabolic, not moral. Fat accumulated through a specific biological process. That process has specific drivers. And those drivers are addressable.
If you were told to monitor it and come back in six months — and left that appointment with no clearer sense of what was actually happening in your liver — the next section is written for that moment.
What This Diagnosis Actually Means for What You Do Next
"Monitor and wait" is not a treatment. It is an observation schedule. It tells you when to measure the condition again. It does not address what is driving the measurement.
The mechanism described above — insulin resistance upregulating de novo lipogenesis, causing the liver to manufacture and retain fat from carbohydrate inputs it cannot process efficiently — has a direct practical implication. The primary drivers of that process are identifiable. Several of them are dietary. Some relate to metabolic patterns the liver has developed over time. None requires a perfect or simultaneous intervention to begin responding. The liver does not require perfection. It requires a reduction in the primary inputs driving fat accumulation and an increase in the inputs that support its ability to export and clear fat.
Three starting points are supported by consistent evidence.
Reduce the primary fructose load. De novo lipogenesis is most strongly activated by excess fructose — not dietary fat, not protein, and not even glucose at equivalent volumes. Fructose is processed almost exclusively by the liver and, under conditions of insulin resistance, is converted directly into triglycerides rather than exported or used for energy. This does not mean eliminating fruit. It means identifying and reducing the concentrated, processed fructose sources that drive the pathway most aggressively: high-fructose corn syrup in packaged foods, sweetened drinks, and ultra-processed products where fructose appears under names that do not advertise what they are. This is a specific and executable starting point. It does not require rebuilding everything at once.
Reduce ultra-processed food exposure. Beyond fructose specifically, ultra-processed foods carry a metabolic burden on the liver that whole foods do not. The research here is consistent and expanding: ultra-processed food intake is independently associated with higher rates of hepatic steatosis and, in some studies, with faster fibrosis progression. The mechanisms are multiple — additives that compromise gut lining integrity, refined carbohydrates that drive repeated insulin spikes, and the near-total absence of the protective polyphenols and fibre compounds found in whole foods that support the liver's oxidative pathways.
Add foods with documented liver fat support. The Mediterranean-pattern eating approach carries the strongest evidence base for liver fat reduction of any dietary framework studied in NAFLD and NASH research. The mechanism involves omega-3 fatty acids — specifically EPA and DHA — polyphenols that reduce hepatic inflammation, and compounds that support the fatty acid oxidation process: the liver's ability to burn fat rather than store it. This is the additive side of the intervention. [Specific foods that support liver fat metabolism](link to P2-01) are covered in the healing foods section of this site, with the mechanism behind each one.
If this helped, here is what helped me first.
The 72-Hour Emergency Protocol. Enter your email and I'll send it now. Free.
One more thing, because it applies to almost everyone at this stage: if the first week goes badly, that is not information about whether this is possible for you. It is information about one week. The mechanism that drove fat accumulation over months or years does not shift direction in seven days. The difficult Tuesday — the bad meal, the week that falls apart — is not the problem. What you tell yourself about it in the days after is where most people actually lose ground. The slip does not have a fixed meaning. The story built on top of it does.
Frequently Asked Questions
Fatty liver disease is a condition in which fat accumulates in more than 5% of liver cells. The non-alcoholic form — NAFLD — affects an estimated 25% of the global adult population and is the most common form of chronic liver disease worldwide. It is not caused by alcohol. It develops through metabolic processes involving how the liver handles carbohydrates and fats when insulin resistance is present. Most people with fatty liver disease have no symptoms.
In people who don't drink heavily, fatty liver develops through metabolic dysfunction. When the liver becomes resistant to insulin, it shifts into a fat-production mode — converting excess carbohydrates, particularly fructose, directly into triglycerides through a process called de novo lipogenesis. This explains why the condition commonly develops in people with no significant alcohol history. Diet composition, metabolic health, and genetic factors are all relevant drivers.
NAFLD (non-alcoholic fatty liver disease) refers to fat accumulation in the liver without significant inflammation. NASH (non-alcoholic steatohepatitis) is the same fat accumulation combined with liver cell inflammation and damage — a more serious stage that carries higher risk of progression to fibrosis and cirrhosis. Standard blood tests cannot reliably distinguish between them; fibroscan or biopsy is required for accurate staging.
Most people with fatty liver disease have no symptoms in the early stages. When symptoms do occur, they can include fatigue, mild discomfort or fullness in the upper right abdomen, and general malaise. Elevated liver enzymes — particularly ALT and AST — are often the first detectable sign, typically found incidentally during routine blood work. The absence of symptoms does not mean the condition is not progressing.
The research on this is consistent: hepatic steatosis responds to specific nutritional and lifestyle changes, particularly when the metabolic drivers are addressed directly. The liver has significant regenerative capacity. Studies and documented individual cases show measurable reductions in liver fat, inflammation, and fibrosis scores. Results vary considerably between individuals, and no single intervention produces the same outcome for everyone. The condition can progress — or it can respond. The difference is largely determined by what drives it and whether those drivers are addressed.
Fatty liver disease is most commonly first identified through elevated liver enzymes in a standard blood panel — ALT and AST are the primary markers. Imaging (ultrasound or MRI) can detect fat deposits in the liver. Fibroscan (transient elastography) measures liver stiffness and provides non-invasive staging of fibrosis. A liver biopsy remains the gold standard for distinguishing simple steatosis from NASH but is not used routinely due to its invasive nature.
The research most consistently supports reducing fructose and ultra-processed food intake, increasing foods associated with lower liver fat accumulation — particularly those found in Mediterranean-pattern eating — and reducing refined carbohydrates that drive de novo lipogenesis. The specific mechanism — addressing insulin resistance and the liver's carbohydrate processing pathways — is more useful than a generic eat-well framework. Food-level research, with the mechanism behind each food, is covered in the healing foods section of this site.
If this was useful, the protocol is where I started. It is free. Get It Here.
Understanding the mechanism is the first step. The 72-Hour Emergency Protocol is the second — it covers the specific first moves I made once I understood what was driving the fat accumulation. Not a program. Not a sales page. A documented starting point. It's free. Start there.
The food and ingredient system for people whose liver numbers still aren't moving.
Get the 72-Hour Emergency Protocol — free
The first step I took when my ALT hit 127. Enter your email and I'll send it now.
Created with ©systeme.io